Mvp Weight Loss Surgery

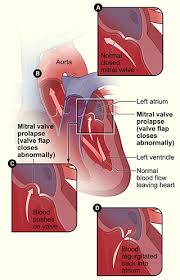
PatientPlus articles are written by UK doctors and are based on research evidence, UK and European Guidelines. They are designed for health professionals to use, so you may find the language more technical than the .Mitral valve prolapse (MVP) is an abnormal bulging of one or both of the mitral valve leaflets into the left atrium during ventricular systole.[1] MVP is defined on echocardiography as single or bileaflet prolapse of at least 2 mm, with or without leaflet thickening.MVP is a common condition and is a risk factor for mitral regurgitation, congestive heart failure, cardiac arrhythmias and infective endocarditis.[1] Myxomatous degeneration is the most common cause of MVP in the USA and Europe.[1] The prevalence of MVP is estimated as 2-3% of the population.[3] However, some studies have found a prevalence of less than 1%.[4] The cause is often multifactorial.A common occurence is leaflet thickening and redundancy, known as myxomatous degeneration - not related to hypothyroidism but involving the accumulation of proteoglycans on histology.

The underlying mechanism is not known.MVP may also occur with histologically normal valves. Contributing/associated factors may be:A disproportionately small left ventricular (LV) cavity.
Country Homes For Sale In Pittsburg KsUnrepaired secundum atrial defects.
Whole House Air Purifier For FurnaceCertain recognised syndromes:Marfan's syndrome;
Blue Cattle Dog Puppies Sale Qldrecent research suggests 28% prevalence (lower than previously thought).Ehlers-Danlos syndrome (6% prevalence).Adult polycystic kidney disease.Genetic factors - there is probably a familial, autosomal dominant condition with variable penetrance and variable clinical presentation. There may be other genetic forms.See also the separate Heart Auscultation article.

MVP is generally asymptomatic, unless there are complications such as significant mitral regurgitation. mon physical features associated with MVP include low body weight, pectus excavatum, hypermobility of joints and arm span greater than height (which may indicate Marfan's syndrome).A careful physical examination is said to be highly sensitive for echocardiographic MVP, although it is not specific. MVP may also be found on echocardiography when auscultation is normal. Classical auscultation findings are as follows:A dynamic mid-to-late systolic click, often followed by a late systolic mitral regurgitant murmur.The murmur is dynamic in that it moves within systole as the loading conditions change.There is an earlier click with reduction of end-diastolic volume - eg, on standing or a Valsalva manoeuvre.The click will be later in systole when the LV afterload or end-diastolic volume is increased - eg, by squatting or hand grips.Symptoms of autonomic dysfunction may occur with genetically inherited MVP - eg, anxiety, panic attacks, palpitations, syncope or presyncope, neuropsychiatric symptoms.

Look for associated conditions - eg, Marfan's syndrome.A click heard during auscultation may also be due to:Redundant leaflets or chordae, without echocardiographic prolapse.Pericarditis.Other causes of mitral regurgitation.Patients with signs of MVP should have 2-D echocardiography. This shows the prolapse and distinguishes it from other causes of systolic clicks.As mentioned above, strict criteria for echocardiographic diagnosis are important to avoid over-diagnosis.Transthoracic echocardiography (TTE) can confirm MVP but can miss prolapse of the lateral scallop of the valve; trans-oesophageal echocardiography (TOE) may be more sensitive. 3-D TOE provides vary accurate localisation of lesions and assessment of valve pathology.[8] ECG and CXR are usually normal unless there has been progression to significant mitral regurgitation. The ECG may show nonspecific ST-segment and T-wave abnormalities.An ambulatory 24-hour ECG monitor may be useful to detect cardiac arrhythmias.If there is doubt about exercise tolerance, an exercise test may be useful.
Patients with MVP can be classified as at high or low risk of developing severe mitral regurgitation.Low riskThose with no symptoms, only mild regurgitation and stable examination findings, do not need treatment. These patients can be followed up conservatively.Symptoms of autonomic dysfunction can be treated with a trial of beta-blockers and abstinence from caffeine, alcohol and cigarettes.Asymptomatic patients with minimal disease can be reassured regarding the benign nature of their condition. If echocardiography shows no clinically significant mitral regurgitation and thin leaflets, follow-up with clinical examination and echocardiography can be arranged every 3-5 years. These patients can continue with a normal, unrestricted lifestyle.High riskFactors which increase the risk of severe mitral regurgitation developing are:Age over 50, hypertension or obesity.Mitral regurgitation during exercise but not at rest.Echocardiographic findings of mitral leaflet thickness >5 mm, posterior leaflet prolapse or increased LV dimensions.

Reduced LV systolic function.Patients at high risk need follow-up to monitor for progressive mitral regurgitation. If this occurs, the surgical repair or replacement of the valve may be needed, and the optimal timing of surgery must be considered.ProphylaxisAntithrombotic treatment is not recommended for MVP alone.Endocarditis prophylaxis:Patients with MVP are at increased risk of endocarditis if they have:A systolic click and murmur on examination.Myxomatous degeneration and mitral regurgitation on echocardiography.'High-risk' features, such as LV dilatation, left atrial enlargement, leaflet thickening, redundant chordae, or other high-risk features, as above.National Institute for Health and Care Excellence (NICE) guidelines state that:[10]Routine antibiotic prophylaxis is not required for most procedures.However, antibiotic cover for infective endocarditis should be given to patients who are receiving antibiotics for a gastrointestinal or genitourinary procedure to an infected site.Patients at risk of endocarditis should be aware of relevant symptoms.

SurgerySymptoms of heart failure, severity of mitral regurgitation, presence or absence of atrial fibrillation, LV systolic function, LV end-diastolic and end-systolic volumes, and pulmonary artery pressure (at rest and with exercise) all influence the decision to recommend mitral valve surgery. Valve surgery is indicated for patients with:Symptomatic severe mitral regurgitation.Patients who are asymptomatic but have LV enlargement (end-systolic diameter >45 mm) or reduced systolic function (ejection fraction <60%).Severe mitral regurgitation with atrial fibrillation or pulmonary hypertension.Surgical options are:Management of MVP may include valve surgery. Mitral valve repair is associated with excellent long-term survival and remains superior to mitral valve replacement.[11] NICE recommends that the evidence for the safety and efficacy of percutaneous mitral valve leaflet repair for mitral regurgitation is currently inadequate.A technique using polytetrafluoroethylene neochordae has been used as an alternative to mitral valve surgery.

The management of asymptomatic patients with severe mitral regurgitation but preserved LV function is controversial. However, there is a trend towards earlier surgical valve repair for patients with severe mitral regurgitation. This is because:There is a high success rate and durability of surgical repair.Some research shows improved clinical outcomes with early intervention.Occult LV dysfunction can precede symptoms.Those with severe mitral regurgitation and a flail valve leaflet may benefit from early surgical repair.Anterior leaflet mitral valve repair is associated with a higher risk for re-operation than posterior leaflet repair.The overall prognosis is excellent for most patients with MVP, with an expected lifespan similar to the general population. A minority of patients may develop complications such as:Progression to severe mitral regurgitation, which may require surgery.A small increased risk of sudden cardiac death:The absolute risk is very low but, in patients with myxomatous MVP, it is twice that of the general population.

If there is severe mitral regurgitation with a flail leaflet, this carries a higher risk (up to 2% per year).A small increased risk of infective endocarditis:Without mitral regurgitation, the incidence of infective endocarditis is similar to that of the general population.In patients with MVP and a systolic murmur, the risk increases to about 0.05% per year.Possibly an increased risk of stroke: The association between the increased prevalence of cerebrovascular events and MVP in young patients without evidence of cerebrovascular disease is unclear.The major risk factors for cerebrovascular events include age older than 50 years, thickened mitral valve leaflets, atrial fibrillation and a need for mitral valve surgery.It has been suggested that first-degree relatives of those with MVP should have echocardiography to screen for the condition.[14] Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. EMIS has used all reasonable care in compiling the information but make no warranty as to its accuracy.